Nutritional management
Effective management of nutrition is recommended as an integral component of education and clinical care for those at risk of developing or living with any type of diabetes. Input from a registered dietitian should be offered to all people living with diabetes and those deemed to be at high risk of developing type 2 diabetes. The following recommendations are adapted from Diabetes UK. These recommendations can be used to develop individualised nutrition and activity plans.
Nutritional recommendations for the prevention of type 2 diabetes
- target weight loss of 5%
- restrict energy intake
- reduce total and saturated fat intake
- increase fibre
- increase physical activity
- include wholegrains, some fruit, green leafy vegetables
- reduction in red and processed meat, potatoes, sugar sweetened beverages and refined carbohydrates (CHO)
- multi component lifestyle interventions which are culturally sensitive to reduce risk in ethnic minority groups.
Recommendations for glycaemic control and type 2 diabetes
- aim for 5% weight loss in those who are overweight by reducing calories consumed and increasing energy expenditure
- aim for a Mediterranean style diet or equivalent
- offer individualised support to identify and quantify CHO intake, encourage low glycaemic index (GI) foods and consider reducing amount of total CHO. Low GI food take longer to breakdown raising blood glucose levels steadily and may be associated with improved HbA1c.

Recommendations for glycaemic control and type 1 diabetes
- education to support people with type 1 diabetes should be offered to identify and quantify dietary and CHO intake for glycaemic control specifically
- adjust insulin to CHO intake in people using multiple daily injections or insulin pumps (carbohydrate counting)
- aim for consistent quantities of CHO on a day-to-day basis in people on fixed insulin regimes.
Further resources
Diabetic foods
People living with diabetes should avoid foods labelled as ‘diabetic’ / ‘suitable for diabetics’ as there is no role or benefit from the use of diabetic foods. ‘Diabetic’ foods have been a feature in many chocolate, sweets, biscuits, and bakery ranges available in a variety of high street outlets such as supermarkets, pharmacies and “health food shops” as well as being widely available on the internet. As ‘diabetic’ foods can be just as high in calories and fat, continued consumption of these foods can contribute to weight gain and increase an individual’s susceptibility to other health conditions, for example, heart disease and stroke (DUK / European Commission).
Carbohydrate counting
While people with type 2 diabetes are taught to be aware of the size of their carbohydrate intake, people with T1DM need a more exact measure called carbohydrate counting. Carbohydrate counting helps them to optimise their blood glucose control by adjusting their insulin doses. CHO can be counted in two ways, in grams or as CHO portions (CP). One CP is usually equal to 10g of carbohydrate.
Insulin-to-carbohydrate ratios (Insulin-CHO ratio) are different from person to person, depending on age, weight, activity levels and how sensitive the person is to insulin.
The diabetes health care team will help the person with T1DM diabetes to work out their insulin-CHO ratio and, eventually, a different ratio may be set for each meal. They will usually estimate the starting insulin-to-carb ratio and then fine-tune this based on blood glucose control.
Once the quantity of CHO of a meal and the insulin-carb ratio are known, then the insulin bolus dose for that meal can be calculated.
If the meal had 70g of carbohydrate and the Insulin -CHO ratio was 1 unit of bolus insulin for every 10g carbohydrate, then seven units would be given for that meal.
The amount taken will also depend on other factors such as current blood glucose level, illness or planned physical activity.
See: BERTIE Type 1 Diabetes Education Programme. BERTIE is a diabetes education course that teaches people with type 1 diabetes how to manage insulin doses, matching them to carbohydrate intake, and live life on a day-to-day basis.
Alcohol
Alcohol in moderate amounts can be enjoyed safely by most people with T1DM and general advice about safe alcohol intake (14 units or less per week) should be applied. However, alcohol intake is associated with an increased risk of hypoglycaemia for those taking insulin. Pragmatic advice for those who wish to continue to consume alcohol would be insulin dose adjustment, additional carbohydrate or a combination of both. Alcohol is contraindicated for those with hypertension, hypertriglyceridemia, some neuropathies, retinopathy and during pregnancy.
For more information, see: Alcohol
Smoking
There is a long established, clear link between smoking and the risk of developing type 2 diabetes due to increasing insulin resistance, caused by cellular damage. Increased insulin resistance caused by smoking, means those with already established type 2 diabetes may require intensification of diabetes medications (including insulin). Persistently elevated blood glucose levels caused by increased insulin resistance, leads to significant long-term complications affecting major organ systems within the body (Joshu and Tibbs, 1999).
People living with diabetes should be encouraged to stop smoking and educated as to the multiple health benefits. People living with diabetes can be referred to the local stop smoking services.
For more information, see: Smoking cessation
Older people with diabetes
Some older persons with diabetes may experience poor nutritional status with physical, social and psychological factors affecting intake. Education should continue to be offered to older persons, including dietary intervention – age should not restrict access. Dietetic input is key to assess nutritional status and formulate individualised care plans which take into account the changes in nutrients that are required as the body ages. Guidelines and care planning should be further adapted for those living with dementia with a focus on maintaining nutritional intake and preventing malnutrition.
Ramadan
Fasting the Holy month of Ramadan constitutes one of the five pillars of the Muslim faith. Although there is some evidence that intermittent fasting during Ramadan may be of benefit in losing weight and cardiometabolic risk factors, there is no strong evidence these benefits apply to people with diabetes. The European Association for the Study of Diabetes consensus recommendations emphasise the importance of patient factors and comorbidities when choosing diabetes medications including the presence of comorbidities, atherosclerotic cardiovascular disease, heart failure, chronic kidney disease, hypoglycaemia risk, weight issues and costs. Structured education and pre-Ramadan counselling are key components to successful management of patients with diabetes. These should cover important aspects like glycaemic targets, self-monitoring of blood glucose, diet, physical activity including Taraweeh prayers, medication and dose adjustment, side effects and when to break the fast.
Children with type 1 diabetes should strongly be advised not to fast due to the high risk of acute complications such as hypoglycaemia and probably diabetic ketoacidosis (DKA), although there is very little evidence that DKA is increased in Ramadan. Pregnant women with diabetes or gestational diabetes should be advised to avoid fasting because of possible negative maternal and foetal outcomes. Hypoglycaemia is a common concern during Ramadan fasting. To prevent hypoglycaemic and hyperglycaemic events, the adoption of diabetes self-management education and support principles are recommended. The use of the emerging technology and continuous glucose monitoring during Ramadan could help to recognize hypoglycaemic and hyperglycaemic complications related to omission and/or medication adjustment during fasting; however, the cost represents a significant barrier (Ibrahim et al, 2020).
Summary guidance for fasting during Ramadan
Structured education programmes
A number of structured education programmes are available for those living with diabetes.
DESMOND
DESMOND - Diabetes education and self-management for ongoing and newly diagnosed - is group-based education which aims to support people with a diagnosis of type 2 diabetes and work with them to self-manage their condition, through a structured education programme to target lifestyle modification and behaviour change which can be culturally adapted. These programmes are delivered virtually or in-person over one whole or two half days.
Content includes:
- thoughts and feelings of the participants around type 2 diabetes
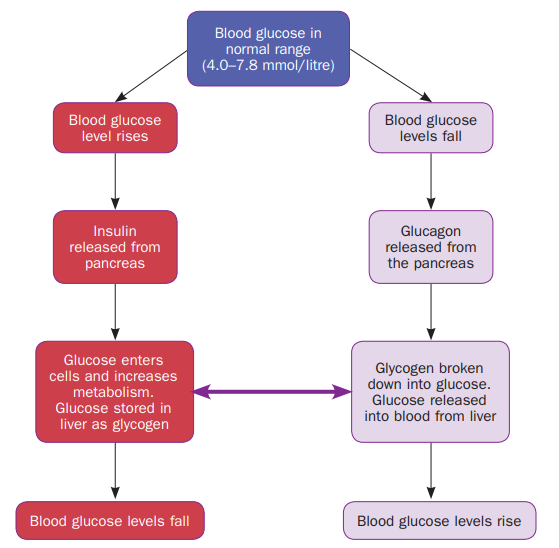
- understanding diabetes and glucose: what happens in the body
- understanding the risk factors and complications associated with diabetes
- understanding more about monitoring and medication
- how to take control – Food Choices – Physical Activity
- planning for the future
DAFNE
DAFNE – Dose adjustment for normal eating, aims to help adults with type 1 diabetes lead as normal a life as possible, whilst also maintaining blood glucose levels within healthy targets, to reduce the risk of long-term diabetes complications. DAFNE educates people with type 1 diabetes about their condition, insulin use and CHO counting.
Education programmes will vary depending on geographical location.
Reversal of type 2 diabetes
Following the DIRECT study, the Type 2 Diabetes Path to Remission Programme (T2DR) has been launched in England. This programme provides a low calorie, total diet replacement treatment for people who are living with type 2 diabetes and obesity or overweight. Eligible participants will be offered low calorie, total diet replacement products including soups and shakes consisting of 800 to 900 kilocalories a day for 12 weeks. During this time, participants will replace all normal meals with these products. See further information here: NHS England
NHS Type 2 Diabetes Path to Remission Programme.
Recommendations for weight management and remission for people living with type 2 diabetes:
- for overweight or obese people with Type 2 diabetes
- for remission, aim for weight loss of 15kg as soon as possible after diagnosis – this may be achieved by total diet replacement or meal replacement plans providing 800-1200 Kcal per day for 12 weeks
- to improve glycaemic control and CVD risk, aim for at least 5% weight loss achieved by reducing calorie intake and increasing energy expenditure.
Physical activity
Increased physical activity is associated with a 25-40% reduction in the relative risk of developing type 2 diabetes (Aune et al, 2015).
Weight management, physical activity and exercise have numerous benefits for people with type 2 diabetes – improving blood glucose control, cardiovascular risk factors and well-being. Target activity should be at least 150 minutes per week of moderate to vigorous physical activity over at least 3 days.
In type 1 diabetes, physical activity can improve cardiovascular fitness leading to a reduction in CVD and mortality. However, there is limited evidence of improved glycaemic outcomes, and whilst exercise will reduce blood glucose levels, it is also associated with increased hypo and hyper glycaemia. For planned exercise, reduction in insulin is the preferred method to prevent a hypo. For unplanned exercise, additional CHO may be required.
Diabetes UK has produced a number of information prescriptions which assist the health care professional to educated the person living with, or at risk of developing diabetes.
For more information, see: Physical activity
Physical activity and lifestyle tips for managing type 2 diabetes
Leicester Diabetes Centre (LDC) has highlighted five important health behaviours people with diabetes should be aware of to help them better manage their condition. These are the five S’s:
Managing type 2 diabetes isn't just about medication – daily habits around movement, exercise, and sleep make a real difference in health and blood glucose levels.
Key points to advise patients
Physical activity and good sleep improve blood glucose, reduce health risks, and support long-term wellbeing for people living with type 2 diabetes. Offer the following advice to patients:
- Take a break from sitting down: Move every 30 minutes to improve blood sugar control. Even simple movements help.
- Add more steps to your day: Adding just 500 extra steps a day can reduce health risks. A brisk 5–6-minute walk daily may add years to your life.
- Improve your sleep: Easier said than done, but aim for consistent, good-quality sleep. Too much or too little sleep, or poor sleep patterns, can make diabetes harder to control.
- Strengthen muscles: Activities like tai chi and yoga are said to improve insulin sensitivity and help manage blood sugars. (Kanaley, J A et al. (2022) Exercise/Physical Activity in Individuals with Type 2 Diabetes: A Consensus Statement from the American College of Sports Medicine, Med Sci Sports Exerc. Feb 1;54(2):353–368.)
- Exercise regularly: Aim for 150+ minutes of moderate or 75+ minutes of vigorous exercise weekly. Don’t let more than two days pass without moving. Combine cardio with strength, flexibility and balance activities.